 |
|||||||
|
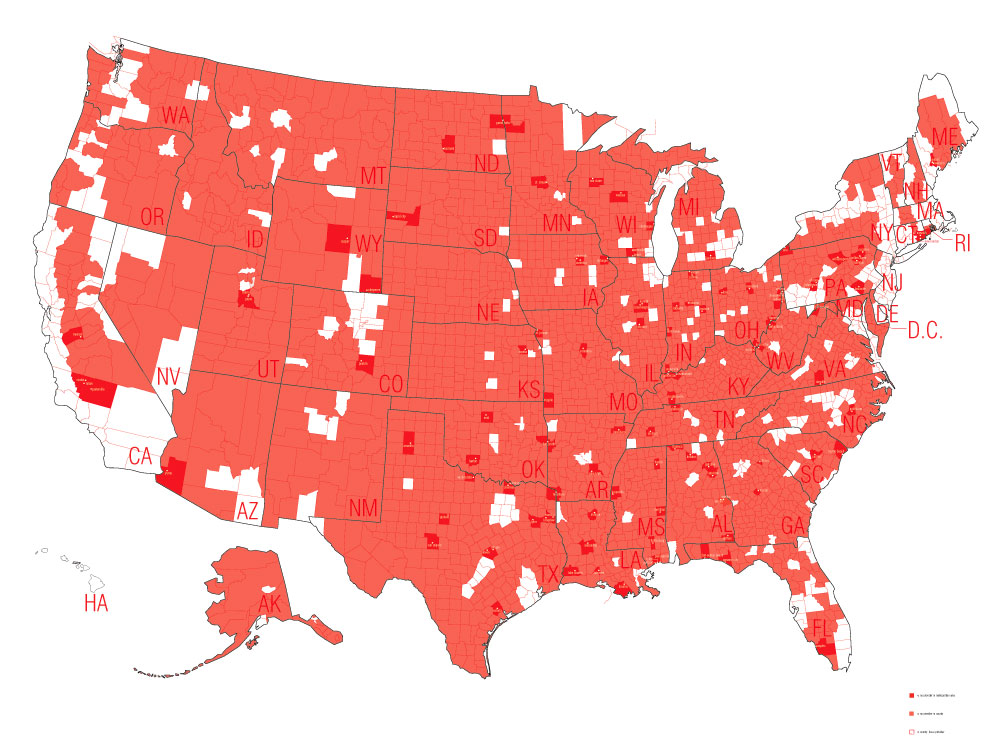
Although Roe v. Wade (1973) remains legally intact, different states independently control and govern degrees of access. According to the Alan Guttmacher Institute, in 20005 87% of U.S. counties had no abortion provider and in non-metropolitan areas, 97% of counties had no provider. Approximately one in four women who have had an abortion are required to travel 50 miles or more for the procedure.* As more restrictive legislation continues to be passed, abortion has become more difficult for certain groups to exercise their legal right granted by federal law. My research explores issues of the first amendment and public space through examining the space of abortion clinics. Politicizing the Female Body illustrates how highly restrictive state legislation makes abortion access next to impossible for many lower income women in states with few providers. Depending upon one’s state of residence, abortion access varies widely. In states such as South Dakota and Mississippi extremely restrictive laws are in place and 98% of the counties are without abortion access. Conversely in states such as Hawaii and New Jersey access is far more open with 100% of the counties in Hawaii and 90% of the counties in New Jersey with providers. The project reveals how legislation creates both landscapes of access and denial. As the political philosopher Iris Marion Young writes, “…[w]omen in sexist society are physically handicapped. Insofar as we learn to live out our existence in accordance with the definition that patriarchal culture assigns to us, we are physically inhibited, confined, positioned, and objectified.”** State abortion legislation is created by legislatures that have no real understanding or relationship to the physical hardships these restrictions inflict upon women. Employing drawing and mapping methodologies, the project makes visually clear the impact state restrictions have on abortion access.
** Iris Marion Young, Chapter 8 Throwing Like a Girl, Throwing Like a Girl and Other Essays in Feminist Philosophy and Social Theory, Bloomington: Indiana University Press, 1990, p.153.
|
|
|||||||
|





